Saturday, May 19, 2018
Saturday, January 13, 2018
Current Methods of Treatment
Current treatment options focus on an aesthetically pleasing and immediate solution; however, inducing bone growth provides a long-lasting, integrative solution. Several biological solutions exist for craniofacial defects with area less than 25cm2. Patients may receive an autograft, which is considered the gold standard of biologic bone replacement, where a piece of bone harvested from various sources in the patient’s body, usually from the fifth to seventh rib or from the ilium of the hip, is restructured to fill the calvarial defect void., While autologously harvested bone decreases the risk of bodily rejection and has high rates of bone fusion, the procedure increases the risk of infection from the graft site, produces multiple incisions which may prolong recovery, and lacks the specific mechanical and geometric properties required to heal the calvarial defect. Similarly, patients may receive grafts from other humans or animals, known respectively as allografts and xenografts. Conversely to the autograft, these grafts have a much higher rate of rejection and more malleable mechanical properties, but do not achieve as high rates of bone fusion. Successful fusion of an allograft or xenograft helps to heal a calvarial defect, but patients may have a lifelong prescription of immunosuppressants to curb the threat of rejection which may lead to greater risks of contracting other illnesses. Synthetic substitutes incorporate a mesh mold covered with polymethyl methacrylate (PMMA) as a personalized mold for the missing skull. Synthetic solutions may have manufactured ideal strength and cosmetic appearance, but lack the integration of bone with the mold and bone growth and have the potential to elicit an immune response for rejection. Larger injuries may require treatment that can structurally handle the load, namely metal meshes which have many of the same positives and negatives of synthetic treatments,.
Current treatment options focus on an aesthetically pleasing and immediate solution; however, inducing bone growth provides a long-lasting, integrative solution. Several biological solutions exist for craniofacial defects with area less than 25cm2. Patients may receive an autograft, which is considered the gold standard of biologic bone replacement, where a piece of bone harvested from various sources in the patient’s body, usually from the fifth to seventh rib or from the ilium of the hip, is restructured to fill the calvarial defect void., While autologously harvested bone decreases the risk of bodily rejection and has high rates of bone fusion, the procedure increases the risk of infection from the graft site, produces multiple incisions which may prolong recovery, and lacks the specific mechanical and geometric properties required to heal the calvarial defect. Similarly, patients may receive grafts from other humans or animals, known respectively as allografts and xenografts. Conversely to the autograft, these grafts have a much higher rate of rejection and more malleable mechanical properties, but do not achieve as high rates of bone fusion. Successful fusion of an allograft or xenograft helps to heal a calvarial defect, but patients may have a lifelong prescription of immunosuppressants to curb the threat of rejection which may lead to greater risks of contracting other illnesses. Synthetic substitutes incorporate a mesh mold covered with polymethyl methacrylate (PMMA) as a personalized mold for the missing skull. Synthetic solutions may have manufactured ideal strength and cosmetic appearance, but lack the integration of bone with the mold and bone growth and have the potential to elicit an immune response for rejection. Larger injuries may require treatment that can structurally handle the load, namely metal meshes which have many of the same positives and negatives of synthetic treatments,.
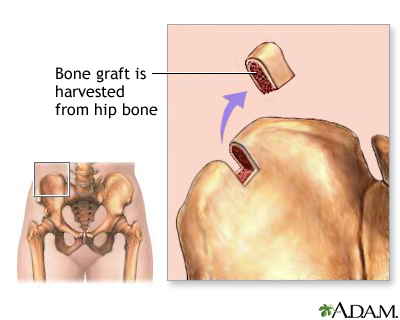


Figure 1 - An autograft (left) and a synthetic mesh (center) are two typical treatment options for typical calvarial defects (right).

Benefits of Personalized Medicine
While the current bone healing market has many treatment options available, all have benefits and faults, namely the risk of an immune response for rejection and a lack of personalized fit for optimal mechanical properties for the calvarial defect.
While the aforementioned solutions all provide adequate treatment for patients with calvarial defects, our stakeholders voiced a concern that personalized medicine provides optimal treatment for patients. Dr. David Eckmann of the Department of Bioengineering and Anesthesiology of the University of Pennsylvania advocated for the benefits of personalized medicine stating that patients respond better to personalized treatment. Dr. Ari Brooks of the University of Pennsylvania Department of Clinical Surgery echoed Dr. Eckmann’s sentiments about personalized medicine, and stated that using cheaper materials such as polycaprolactone (PCL) to develop the scaffold will make the treatment less expensive without taking away from the benefits. Personalized medicine and low cost treatment extend well beyond the scope of this course, and ideally, our project will provide better treatment for a lower cost to people around the globe with calvarial defects.
Evaluation Methods

Our review of the current treatment market and the advice of our stakeholders helped our team identify the problem with current treatment: no treatment combines personalized medicine with autologous bone growth and decreases the risk of infection and rejection. Current bone graft methods have insufficient mechanical and biochemical properties, pain at both the implementation and derived sites, rejection rates in up to 30% of procedures, rates of infection up to 10% in patients, and improper geometry to match that of the calvarium.,,,, Metal and PMMA-based implants have similar issues in terms of infection, mechanical strength, degradation, and potential multiple procedures. The current treatments, while effective to a certain degree, do not provide total patient care with a personalized approach and bone regeneration.
Radiologists will administer some form of imaging to diagnose a calvarial defect properly usually with either magnetic resonance imaging (MRI) or computed tomography (CT). CT stands as the most reliable imaging technique because of the high contrast between bone and native tissue. Our patient treatment process will begin with creating multiple transverse two-dimensional images of the patient’s skull which compile into a three-dimensional representation of the patient’s skull. The radiologist obtains the CT files as a stack of DICOM images, which the user will input into a MatLab algorithm. Our algorithm will use a slice-by-slice reconstruction software to re-create a three-dimensional image of calvarial defect. A 3D printer will take the reconstruction information and will print the respective porous PCL-based scaffold that will optimally fit into the defected skull. The clinician will implant pre-osteoblast and growth factor loaded scaffold back into the native skull to stimulate bone regrowth within the scaffold and native skull. The overall process will take time, but the patient will have native bone regeneration into a complete skull.
Our solution creates a uniform patient-treatment pipeline that produces personalized outputs. Native calvarial bone regrowth is the ultimate end goal of this project, but current advances in tissue engineering have already proven the possibility of regeneration of parietal bone in rat models. The major innovation in this solution is through the creation of a reconstruction pathway that simply requires an input of 3D-CT images and produces an output of a personalized scaffold that stimulates the aforementioned bone regeneration with a manufactured drug release profile. This well-defined pathway will allow for greater patient outcome and less variability in treatment of patients.
Monday, January 8, 2018

Problem Statement
Over 100,000 patients receive a cranioplasty each year, and
many of these patients could benefit from a more robust treatment method.
Therefore, we propose a novel, personalized treatment regimen for patients with
craniofacial injuries specifically of the calvarial bone. Our project consists
of the two following aims: developing a personalized scaffold to place in the
calvarial defect and optimizing scaffold drug delivery of growth factors and
biologics for sustained release profiles and eventual growth of native bone
tissue within the defect. This treatment method will produce a streamlined,
personalized process for native bone growth in patients with calvarial defects.
Solution


The above image shows the overall pipeline of our project. Initially, a patient with a craniofacial defect will undergo CT or MRI imaging so the attending physician can understand the physical extent of the injury in terms of general size, location, and shape. The 3D file of the traced skull obtained from the imaging will export to MATLAB as a stack of DICOM images. A MatLab algorithm will determine the appropriate volume for the calvarial defect from the input images, and produce an output containing the spatial analysis. Afterwards, .STL file containing the 3D stack of images will output to a CAD workstation for 3D printing. The PCL/MSN scaffold will print according to the dimensions determined from the reconstruction portion.
Biologically, the scaffold with optimal porosity and mechanical strength will print for the calvarial defect. The scaffold will bear the several growth factors and pre-osteoblast mesenchymal stem cells (MSCs) loaded in its pores. After biological seeding, a quick surgical procedure will implant the scaffold in the calvarial defect to reduce risk of infection. The scaffold will promote native bone tissue regrowth within the skull while the PCL component degrades and engages the manufactured release profile of the growth factors.

Deliverables

Remaining Challenges

Objectives & Approach Overview
Our review of the current treatment market and the advice of our stakeholders helped our team identify the problem with current treatment: no treatment combines personalized medicine with autologous bone growth and decreases the risk of infection and rejection. Current bone graft methods have insufficient mechanical and biochemical properties, pain at both the implementation and derived sites, rejection rates in up to 30% of procedures, rates of infection up to 10% in patients, and improper geometry to match that of the calvarium.,,,, Metal and PMMA-based implants have similar issues in terms of infection, mechanical strength, degradation, and potential multiple procedures. The current treatments, while effective to a certain degree, do not provide total patient care with a personalized approach and bone regeneration.
Radiologists will administer some form of imaging to diagnose a calvarial defect properly usually with either magnetic resonance imaging (MRI) or computed tomography (CT). CT stands as the most reliable imaging technique because of the high contrast between bone and native tissue. Our patient treatment process will begin with creating multiple transverse two-dimensional images of the patient’s skull which compile into a three-dimensional representation of the patient’s skull. The radiologist obtains the CT files as a stack of DICOM images, which the user will input into a MatLab algorithm. Our algorithm will use a slice-by-slice reconstruction software to re-create a three-dimensional image of calvarial defect. A 3D printer will take the reconstruction information and will print the respective porous PCL-based scaffold that will optimally fit into the defected skull. The clinician will implant pre-osteoblast and growth factor loaded scaffold back into the native skull to stimulate bone regrowth within the scaffold and native skull. The overall process will take time, but the patient will have native bone regeneration into a complete skull.
Our solution creates a uniform patient-treatment pipeline that produces personalized outputs. Native calvarial bone regrowth is the ultimate end goal of this project, but current advances in tissue engineering have already proven the possibility of regeneration of parietal bone in rat models. The major innovation in this solution is through the creation of a reconstruction pathway that simply requires an input of 3D-CT images and produces an output of a personalized scaffold that stimulates the aforementioned bone regeneration with a manufactured drug release profile. This well-defined pathway will allow for greater patient outcome and less variability in treatment of patients.
Evaluation Methods
Our review of the current treatment
market and the advice of our stakeholders helped our team identify the problem
with current treatment: no treatment combines personalized medicine with
autologous bone growth and decreases the risk of infection and rejection.
Current bone graft methods have insufficient mechanical and biochemical
properties, pain at both the implementation and derived sites, rejection rates
in up to 30% of procedures, rates of infection up to 10% in patients, and
improper geometry to match that of the calvarium.,,,, Metal and
PMMA-based implants have similar issues in terms of infection, mechanical
strength, degradation, and potential multiple procedures. The current
treatments, while effective to a certain degree, do not provide total patient
care with a personalized approach and bone regeneration.
Radiologists will administer some form
of imaging to diagnose a calvarial defect properly usually with either magnetic
resonance imaging (MRI) or computed tomography (CT). CT stands as the most reliable
imaging technique because of the high contrast between bone and native tissue.
Our patient treatment process will begin with creating multiple transverse
two-dimensional images of the patient’s skull which compile into a
three-dimensional representation of the patient’s skull. The radiologist
obtains the CT files as a stack of DICOM images, which the user will input into
a MatLab algorithm. Our algorithm will use a slice-by-slice reconstruction
software to re-create a three-dimensional image of calvarial defect. A 3D
printer will take the reconstruction information and will print the respective
porous PCL-based scaffold that will optimally fit into the defected skull. The
clinician will implant pre-osteoblast and growth factor loaded scaffold back into
the native skull to stimulate bone regrowth within the scaffold and native
skull. The overall process will take time, but the patient will have native
bone regeneration into a complete skull.
Our solution creates a uniform
patient-treatment pipeline that produces personalized outputs. Native calvarial
bone regrowth is the ultimate end goal of this project, but current advances in
tissue engineering have already proven the possibility of regeneration of
parietal bone in rat models. The major innovation in this solution is through
the creation of a reconstruction pathway that simply requires an input of 3D-CT
images and produces an output of a personalized scaffold that stimulates the
aforementioned bone regeneration with a manufactured drug release profile. This
well-defined pathway will allow for greater patient outcome and less
variability in treatment of patients.
Plan for
Demonstrating Feasibility - Key Deliverables:
Personalized 3D
Scaffold: The 3D printed scaffold using the reconstructed file generated
from the optimization algorithm with the PCL-MSN solution will serve as our
first main deliverable. Demonstrating the feasibility of the construct will
start with obtaining publicly-available skull CT images that contain
craniofacial defects. The initial algorithm will use the CT images as a test
input, and then evaluate the accuracy of the computer-generated defects. Our
team will subject the optimized scaffold to physical tests by creating a scaffold
for a mock, medical-grade skull. The CT scan analysis will generate the solid,
3D outline of the specific defect., and SolidWorks will use the 3D outline as
an input where the hollow interior will be replaced with repeated units of the
ideal cross-sectional dimensions to maximize porosity without sacrificing
mechanical strength. Upon examining the resulting design by overlaying the
model into the original CT stack to ensure proper fit, the construct will be
printed using the standard MakerBot. The Department of Mechanical Engineering
and Applied Mechanics has available printers that like the ProJet 6000HD, which
are able to print layer-by-layer with an accuracy of 0.025-0.05mm. As it is
affordable and accessible, one of these high-resolution printers will be
utilized to guarantee scaffold resolution of less than 1mm. Once printed, the
scaffold will be tested for optimal release kinetics, mechanical properties,
and overall fit inside the model skull.
Optimal Mechanical
Properties: During the algorithm optimization phase, mechanical testing of
the PCL-MSN polymer will be occurring simultaneously. The ideal deliverable
through this testing will be that the scaffold itself is able to meet the
minimal acceptable mechanical strength profiles of native bone and other
clinically-approved scaffolds. First, Dynamic Mechanical Analysis (DMA) will be
conducted with an Instron machine to generate a stress-strain curve in addition
to modeling creep and stress-relaxation - all of which will provide information
about the elastic modulus of the scaffold. The Instron machine will also be
used to test the Ultimate Compressive Strength (UCS) of the material. We will
test different compositions depending on PCL-MSN ratios and different levels of
porosity to ensure the device is able to meet the desired mechanical
thresholds. To measure these different levels of porosity, we will utilize a
Scanning Electron Microscopy (SEM). This technique generates high resolution
images by focusing electron particles at the outer surface of the scaffold.
With these images, the size and percent porosity of the scaffold can be
calculated and verified to better optimize the relationship between mechanical
strength and porosity.
Chemical Testing: The first drug
release profiles that will be observed are the antibiotics vancomycin and
moxifloxacin, which are commonly used to treat bacterial infections in bones
and joints. Because the scaffold are intended for clinical applications to
treat cranial defects while overcoming the major drawbacks of current solutions
such as high rates of infection, a significant overarching goal is to
characterize antibody release profiles as accurately as possible. These drugs
will be loaded within the xerogel of the construct for a slow-release profile
over the course of 10 weeks to model the time period required for bone
regeneration and scaffold degradation. Optimal loading profiles for these drugs
will also be monitored to ensure the concentration never reaches an unsafe
level as this could lead to negative side effects such as nephrotoxicity and
ototoxicity. In-vitro studies using MSCs seeded on the 3D printed
material will be conducted to ensure these proper release profiles by assessing
cell viability, cell proliferation, and increased levels of bone regeneration
as described in “Biological Testing”. Immunosuppressant drugs, such as
cyclosporine A, will also be analyzed in a similar manner to limit initial
immune response to the scaffold. Grafts and synthetic scaffolds often fail due
to the high rates of rejection, so implanting the scaffold with these
immunosuppressants will lead to greater mechanical strength of the scaffold and
more sustained bone growth.
Biological Testing: MC3T3 cells are
mouse osteoblast cells, which will be cultured onto the scaffold through two
methods: (1) seeding after the PCL scaffold is printed and placed in a xerogel
solution, or (2) direct seeding through bioprinting with cells in the same
solution as the PCL:MSN, which will then be fed through the 3D printer. The
latter mode of embedding cells has been explored by many labs, including that
of Dr. Jason Burdick of the Department of Bioengineering. In order to ensure
homogeneity, high retention rate, and direct integration within the
macroenvironment, cells can be 3D printed in a cell culture hood. However,
indirect seeding is beneficial in that cells naturally bind to PCL due to its
intrinsic properties, and the viability would be higher than rough injection
due to the large quantity of cells killed during printing. Cytotoxicity is a significant
factor in determining if the 3D printed scaffolds are a viable alternative to
the currently used materials - many metal scaffolds eventually fail.
Experiments such as the LDH and MTS assays can be utilized to understand the
viability of the cells and the cytotoxicity of the environment. For MTS assays,
it is known that proliferating and viable cells reduce the concentration of MTS
tetrazolium when exposed, so a high level of colorized MTS indicates high
degrees of cytotoxicity. Therefore, these results are the most important in
proving the feasibility of the project, as negative results would necessitate
the reevaluation of every aspect of the scaffold to determine the limiting
factor.
Current Progress:
Reconstruction: In terms of the
reconstruction efforts so far, we have been able to make some major
improvements that will allow for less required work next semester. First, we
were able to access publicly-available CT images online and download several
sets of .dicom images of healthy skulls. With this data, we have been able to
successfully read-in 3D CT and separate images on a slice-by-slice basis for
reconstruction. Within these individual slices, we have been able to make
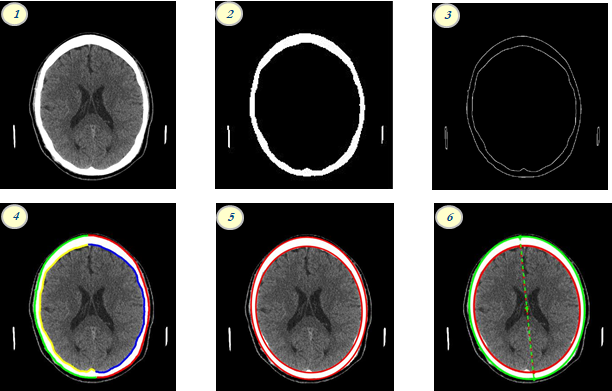
significant progress in our reconstruction efforts. As seen in the image, the
progress to this point can be visualized in six steps. (1) shows our ability to
read in CT data on a slice-by-slice basis for reconstruction. Step (2) shows a
conversion of the CT image to binary, using the most sensitive possible
threshold, which was advised by Dr. Ari Brooks. Image panes (3) and (4) show
our capabilities to create outlines of the skull depending on different borders
and sides of the skull, which will be helpful when localizing defects in 2D.
(5) represents current geometrical modelling that we have employed by using
code to fit an ellipse to the inner and outer borders of the skull through a
least-squares regression. Finally, (6) shows that, with these geometrical
models, we can determine certain properties of the skull, such as the labeled
axis of rotation.
Biologics: Biologically, we accomplished one of the important principle
synthesis reactions necessary for our scaffold’s manufactured drug release
profile: fabrication of blank mesoporous silica nanoparticles. We mimicked a
method developed by Sanjib Bhattacharyya, Henson Wang, and Paul Ducheyne as
detailed in “Polymer-Coated Mesoporous Silica Nanoparticles for the Controlled
Release of Macromolecules” in Acta Biomaterialia. Citation/footnote
(I have paper). First, C18TAB
(octadecyltrimethylammoniumbromide) was dissolved in distilled water at 75℃, and then mixed with 2M NaOH (sodium hydroxide) to make a basic
solution with pH 12. The main molecule, TEOS (tetraethylorthosilicate) was
dissolved in with drops of TESPA (3-(triethoxlysilyl) propyl-succinic
anhydride), and the solution was left to dry for two days. The dried MSN
particles were added to aqueous DMH (dimethylhexadecylamine), stirred, and then
heated. The leftover solid was rinsed with methanol first, followed by rinses
with ethanol and water. This procedure creates pore-expanded, unloaded MSN
particles which can take on a biologic to load its pores when we design
the PCL/MSN solution. The figure Number(MSN stages graphic, obtained from
paper) above shows the main stages of the MSN fabrication and loading
process with the last step of the PEG-coated MSN as the final product necessary
to produce the manufactured drug release profile.



Specifications
Specifications:


Design
Goals, Tradeoffs and Constraints:
Mechanical
Properties: The personalized implant scaffold will be fabricated with a Young’s Modulus >= 2.86GPa and an
ultimate compressive strength (UCS) >=70MPa. Clinical studies have
shown that the ‘gold standard’ procedure for craniofacial reconstruction, the
autograft with bone sourced from parietal bone, has exhibited a Young’s modulus
ranges from approximately 0.9 to 15.54 GPa and an average UCS of 100MPa,,,,. Further studies indicate
that cranial implants experience additional degenerative forces: internal
pressure caused by tensile forces within the skull that range from 80-100kPa,
external pressures caused by impacts to the skull, and pressure applied by the
skin, which results in both shear and tensile forces. These mechanical
properties vary within the calvarial bone depending on several factors (eg.
loading speed, location within calvarium bone, skull thickness, age, etc.), but
human skulls rarely experience these instantaneous pressure changes of these
magnitudes. The scaffold should have the appropriate mechanical properties to
withstand these forces and pressures, but patients with the scaffold should
limit exposure to excessive external forces on the skull.
Currently, PMMA-based
cements (among other synthetic treatment options) have shown that pure
PMMA-based cements have a Young’s Modulus of around 2.86GPa and a UCS of
approximately 93.0MPa,. When we reached out to our stakeholders, Dr. Brooks advised our
team that the mechanical properties of the scaffold do not need to equal those
of autologous bone growth, but must display enough strength so that the
scaffold can withstand the surgical procedure for implantation and maintain the
structural integrity of filling the calvarial bone.
Porosity: The personalized implanted
scaffold will have an average porosity of 60-90%. Studies show that
porosity of 60-90% provides the optimal range for seeding the scaffold with
cells, drugs, growth factors, and other biologics. The pores must be
interconnected to develop and maintain a vascular system required for continued
bone development,,. We will optimize the ideal percent porosity
when we run mechanical testing due to the inverse relationship between porosity
and mechanical strength. No major “trade-offs” will be made, as we will,
ideally, pick the most porous material that is able to meet the minimal limit
of the defined mechanical strength properties. Additionally, the average pore
size for all pores within the generated scaffold will fall between 200 to 350µm
in diameter, and no pore will have a pore size of 150µm or smaller due to the
risks of improper seeding and release of pre-osteoblast cells. Small pores
allow the biologics and growth factors to seed initially in the scaffold, but
will allow also for vascularization and ossification within the pores to ensure
proper bone growth.
Reconstruction: Critical-sized cranial defects will be reconstructed into a 3D
CAD model from a stack of axial CT images. As previously stated, we will
initially limit the scope of the project to only the calvarium of the skull,
which incorporates two major bones: the parietal bone and the frontal bone.
Other bones do not clearly reflect the ovular shape of the skull in axial CT,
so reconstruction will require more advanced algorithms. With the
reconstruction itself, we will be able to take any patient’s 3D-CT stack and
produce a personalized output within a matter of minutes. Specifically, we will
develop the capacity to load in any stack of .DICOM files corresponding to
3D-CT images supplied by a radiologist. Individual slices will then be analyzed
from the stack, and with this data, an algorithm will be developed to identify
and trace the missing section of skull within a single slice. These
individually-corrected slices will then be compiled into a 3D stack and
exported as a CAD-compatible .STL file.
Reconstruction Accuracy: Within each cross-section, modeled data points will be plotted
along the peripherals of the skull geometry (inner and outer borders), with a
minimum accuracy of 90%. By outlining the skull with thousands of data
points, we will fit an ellipse, among other geometrical figures, to these data
points and estimate the skull geometry to this high accuracy for reliable
reconstruction. Although ellipses will likely not be used as the final
reconstruction geometry, these data points are fit through a least-squares
regression to minimize the distance from the borders of the skull to the
implant. Within a single cross-section, the plotted data will be scaled
to accurately resemble the true dimensions of the patient’s skull. Data
points within the CT-images will not be true dimensions of the patient’s skull,
so the algorithm will utilize a scale bar within the CT slices to ensure the
scaffold has the correct dimensions when printed.
3D Printing: When compiling the two-dimensional cross sections of the CT
slices, the third dimension in the superior direction of the axial plain will
have a slice thickness of <1.5mm. Although CT scans of the smallest
clinically feasible slice thickness of the skull, 0.625mm are ideal, studies
have shown that CT slice thickness <1.5mm showed no significant difference
in quantitative properties (eg. volume, surface area) of the skull. Images
acquired at a thickness greater than 1.5mm have demonstrated significantly
different reconstruction values, so they will be avoided for the purposes of
clinical feasibility. The average height of 3D-printed PLA is 400 µm, so we anticipate the resulting constructs
will fall within a standard deviation of 400 µm
due to the major limiting factor of low resolution of the CT scanner itself.
Constraints: For the scope of this project, the primary constraint is the
budget. Due to the pre-set budget of $600, the magnitude and selection of
technology, material, and testing are limited. Specifically, it is particularly
expensive to gain access to imaging modalities such as CT or MRI within the
School of Medicine and Singh Nanotechnology, to buy specific growth factors.
Secondly, there are significant time constraints for the entirety of the
project, as we will not be able to conduct many of the assays we hope to prove
feasibility. Ideally, the implant will go through the inchoate prototype stage
followed by the first round of dry evaluation and in-vitro testing.
However, the fast-approaching deadline limits the project to the prototyping
and, if even possible, simpler in-vitro testing. This rudimentary
testing will allow us to evaluate the proof-of-concept and feasibility;
however, the deadline inhibits the project from proceeding to advanced in-vitro,
ex-vivo, or in-vivo testing stage, where the majority of the
biological feasibility work would occur. Finally, limited meeting times between
group members and our advisors is a constraint that we face. We would like to
be able to brainstorm with our advisors and each other on a more frequent basis
than what scheduling has so-far allowed.
Regulatory Pathway: Our advisor has several years of experience dealing with United
States and European regulatory committees in the field of medical device
production, so we are confident that the physical biomaterials used in this
project would qualify for the 510(k) regulatory pathway within the FDA as a
Class-II medical device. So long as the material used is deemed “substantially
equivalent” to other clinically-approved products such as PMMA-based scaffolds,
then the PCL/Xerogel-based substance will likely be approved with various
biologics and drugs. As discussed previously, there exists a number of
implantable scaffolds for the application of craniofacial reconstruction,
although few are largely-composed of 3D-printed biological material. Thus,
there is a possibility that the overall treatment pathway will require
Pre-Market Approval (PMA) from the FDA due to the invasiveness during
implantation and potential direct human injury with its use. That is, the
scaffold itself would likely only required 510(k) approval due to similarities
with other devices currently available. However, the overall treatment pathway
which utilizes the scaffold will require PMA. Additionally, the FDA is
generally known to be wary of algorithm-based clinical treatment due to the
lack of human overview of the device. Therefore, in producing this device, it
is likely that large-scale randomized, controlled trials will need to be run in
comparing the efficacy of the proposed treatment pipeline compared to current
clinical standards.
[1] https://www.fda.gov/downloads/RegulatoryInformation/Guidances/ucm126054.pdf
[2]https://www.fda.gov/downloads/BiologicsBloodVaccines/GuidanceComplianceRegulatoryInformation/Guidances/Tissue/ucm062592.pdf
Subscribe to:
Posts (Atom)